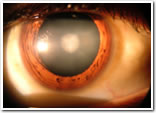
A cataract is a clouding that develops in the crystalline lens of the eye or in its envelope, varying in degree from slight to complete opacity and obstructing the passage of light. Early in the development of age-related cataract the power of the lens may be increased, causing near-sightedness (myopia), and the gradual yellowing and opacification of the lens may reduce the perception of blue colours. Cataracts typically progress slowly to cause vision loss and are potentially blinding if untreated.
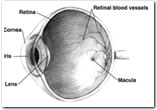
Human eye cross-sectional view, showing position of human lens.
A senile cataract, occurring in the aged, is characterized by an initial opacity in the lens, subsequent swelling of the lens and final shrinkage with complete loss of transparency.[2] Moreover, with time the cataract cortex liquefies to form a milky white fluid in a Morgagnian cataract, which can cause severe inflammation if the lens capsule ruptures and leaks. Untreated, the cataract can cause phacomorphic glaucoma. Very advanced cataracts with weak zonules are liable to dislocation anteriorly or posteriorly. Such spontaneous posterior dislocations (akin to the historical surgical procedure of couching) in ancient times were regarded as a blessing from the heavens, because some perception of light was restored in the cataractous patients.
Causes
Cataracts develop from a variety of reasons, including long-term ultraviolet exposure, exposure to radiation, secondary effects of diseases such as diabetes, hypertension and advanced age; they are usually a result of denaturation of lens proteins. Genetic factors are often a cause of congenital cataracts and positive family history may also play a role in predisposing someone to cataracts at an earlier age, a phenomenon of "anticipation" in pre-senile cataracts. Cataracts may also be produced by eye injury or physical trauma. A study among Icelandair pilots showed commercial airline pilots as three times more likely to develop cataracts than people with non-flying jobs. This is thought to be caused by excessive exposure to radiation coming from outer space. Cataracts are also unusually common in persons exposed to infrared radiation, such as glassblowers who suffer from "exfoliation syndrome". Exposure to microwave radiation can cause cataracts.
For other uses, see Cataract (disambiguation).
Glaucoma
Glaucoma is a group of diseases of the optic nerve involving loss of retinal ganglion cells in a characteristic pattern of optic neuropathy. Although raised intraocular pressure is a significant risk factor for developing glaucoma, there is no set threshold for intraocular pressure that causes glaucoma. One person may develop nerve damage at a relatively low pressure, while another person may have high eye pressure for years and yet never develop damage. Untreated glaucoma leads to permanent damage of the optic nerve and resultant visual field loss, which can progress to blindness.
Glaucoma has been nicknamed "sneak thief of sight" because the loss of visual field often occurs gradually over a long time and may only be recognized when it is already quite advanced. Once lost, this damaged visual field can never be recovered. Worldwide, it is the second leading cause of blindness. Glaucoma affects one in two hundred people aged fifty and younger, and one in ten over the age of eighty.
Pathophysiology
The major risk factor for most glaucomas and focus of modelling and treatment is increased intraocular pressure. Intraocular pressure is a function of production of liquid aqueoushumor by he ciliary body of the eye and its drainage through the trabecular meshwork. Aqueous humor flows from the ciliary bodies into the posterior chamber, bounded posteriorly by the lens and the zonule of Zinn and anteriorly by the iris. It then flows through the pupil of the iris into the anterior chamber, bounded posteriorly by the iris and anteriorly by the cornea. From here the trabecular meshwork drains aqueous humor via Schlemm's canal into scleral plexuses and general blood circulation. The pathology of intraocular hypertension is mostly based on drainage problems through the trabecular meshwork and Schlemm's canal. In primary closed angle glaucoma narrowing of the iridocorneal angle or filtration angle is associated with poor drainage.
The inconsistent relationship of glaucomatous optic neuropathy with ocular hypertension has provoked hypotheses and studies on anatomic structure, eye development, nerve compression trauma, optic nerve blood flow, excitatory neurotransmitter, trophic factor, retinal ganglion cell/axon degeneration, glial support cell, immune, and aging mechanisms of neuron loss.
Diagnosis
Screening for glaucoma is usually performed as part of a standard eye examination performed by ophthalmologists and optometrists. Testing for glaucoma should include measurements of the intraocular pressure via tonometry, changes in size or shape of the eye, anterior chamber angle examination or gonioscopy, and examination of the optic nerve to look for any visible damage to it, or change in the cup-to-disc ratio and also rim appearance and vascular change. A formal visual field test should be performed. The retinal nerve fiber layer could be assessed with statistical imaging techniques such as optical coherence tomography (OCT), scanning laser polarimetry (GDx), and/or scanning laser ophthalmoscopy or Heidelberg Retina Tomography (HRT3). Owing to the sensitivity of some methods of tonometry to corneal thickness, methods such as Goldmann tonometry should be augmented with pachymetry to measure the cornea thickness. While a thicker-than-average cornea can cause a false-positive warning for glaucoma risk, a thinner-than-average cornea can produce a false-negative result. A false-positive result is safe, since the actual glaucoma condition will be diagnosed in follow-up tests. A false-negative is not safe, as it may suggest to the practitioner that the risk is low and no follow-up tests will be done. Examination for glaucoma also could be assessed with give more attention to sex, race, history of drugs use, refraction, inheritance and family history.
Contact lens
A contact lens (also known simply as a "contact") is a corrective, cosmetic, or therapeutic lens usually placed on the cornea of the eye. Modern soft contact lenses were invented by the Czech chemist Otto Wichterle, who also invented the first gel used for their production.
Contact lenses usually serve the same corrective purpose as conventional glasses, but are lightweight and virtually invisible—many commercial lenses are tinted a faint blue to make them more visible when immersed in cleaning and storage solutions. Some cosmetic lenses are deliberately colored to alter the appearance of the eye.
It has been estimated that 125 million people use contact lenses worldwide (2%),[1] including 28 to 38 million in the United States[1][2]and 13 million in Japan.[3] The types of lenses used and prescribed vary markedly between countries, with rigid lenses accounting for over 20% of currently-prescribed lenses in Japan, Netherlands and Germany but less than 5% in Scandinavia.
People choose to wear contact lenses for various reasons.[4] Many consider their appearance to be more attractive with contact lenses than with glasses[citation needed]. Contact lenses are less affected by wet weather, do not steam up, and provide a wider field of vision. They are more suitable for a number of sporting activities.[5] Additionally, ophthalmological conditions such as keratoconus and aniseikonia may not be accurately corrected with glasses.
Types of contact lenses
Corrective contact lenses
A corrective contact lens is a lens designed to improve vision. In many people, there is a mismatch between the refractive power of the eye and the length of the eye, leading to a refraction error. A contact lens neutralizes this mismatch and allows for correct focusing of light onto the retina. Conditions correctable with contact lenses include near (or short) sightedness (myopia), far (or long) sightedness (hypermetropia), astigmatism and presbyopia. Contact wearers must usually take their contacts out every night or every few days, depending on the brand and style of the contact. Recently there has been renewed interest in orthokeratology, the correction of myopia by deliberate overnight flattening of the cornea, leaving the eye without contact lens or eyeglasses correction during the day.
For those with certain color deficiencies, a red-tinted "X-Chrom" contact lens may be used. Although the lens does not restore normal color vision, it allows some colorblind individuals to distinguish colors better.
ChromaGen lenses have been used and these have been shown to have some limitations with vision at night although otherwise producing significant improvements in colour vision. An earlier study showed very significant improvements in colour vision and patient satisfaction
Later work that used these ChromaGen lenses with dyslexics in a randomised, double-blind, placebo controlled trial showed highly significant improvements in reading ability over reading without the lenses This system has been granted FDA approval in the United States, which is reassuring to patients.
Cosmetic contact lenses
A cosmetic contact lens is designed to change the appearance of the eye. These lenses may also correct the vision, but some blurring or obstruction of vision may occur as a result of the color or design. In the United States, the FDA frequently calls non-corrective cosmetic contact lenses decorative contact lenses.
Theatrical contact lenses are a type of cosmetic contact lens that are used primarily in the entertainment industry to make the eye appear pleasing, unusual or unnatural in appearance, most often in horror and zombie movies, where lenses can make one's eyes appear demonic, cloudy and lifeless, or even to make the pupils of the wearer appear dilated to simulate the natural appearance of the pupils under the influence of various illicit drugs.
Scleral lenses cover the white part of the eye (i.e. sclera) and are used in many theatrical lenses. Due to their size, these lenses are difficult to insert and do not move very well within the eye. They may also hamper the vision as the lens has a small area for the user to see through. As a result they generally cannot be worn for more than 3 hours as they can cause temporary vision disturbances.
Similar lenses have more direct medical applications. For example, some lenses can give the iris an enlarged appearance, or mask defects such as absence (aniridia) or damage (dyscoria) to the iris.
Although many brands of contact lenses are lightly tinted to make them easier to handle, cosmetic lenses worn to change the color of the eye are far less common, accounting for only 3% of contact lens fits in 2004.
Therapeutic contact lenses
Soft lenses are often used in the treatment and management of non-refractive disorders of the eye. A bandage contact lens protects an injured or diseased cornea from the constant rubbing of blinking eyelids thereby allowing it to heal. They are used in the treatment of conditions including bullous keratopathy, dry eyes, corneal ulcers and erosion, keratitis, corneal edema, descemetocele, corneal ectasis, Mooren's ulcer, anterior corneal dystrophy, and neurotrophic keratoconjunctivitis. Contact lenses that deliver drugs to the eye have also been developed.
By constructional material
Contact lenses, other than the cosmetic variety, become almost invisible once inserted in the eye
The first contact lenses were made of glass, which caused eye irritation, and were not wearable for extended periods of time. But when William Feinbloom introduced lenses made from polymethyl methacrylate (PMMA or Perspex/Plexiglas), contacts became much more convenient. These PMMA lenses are commonly referred to as "hard" lenses (this term is not used for other types of contacts).
However, PMMA lenses have their own side effects: no oxygen is transmitted through the lens to the cornea, which can cause a number of adverse clinical events. In the late 1970s, and through the 1980s and 1990s, improved rigid materials—which were also oxygen-permeable—were developed. Collectively, these polymers are referred to as rigid gas permeable or 'RGP' materials or lenses. One advantage of hard lenses is that, due to their non-porous nature, they do not absorb chemicals or fumes. The absorption of such compounds by other types of contacts can be a problem for those who are routinely exposed to painting or other chemical processes.
Rigid lenses offer a number of unique properties. In effect, the lens is able to replace the natural shape of the cornea with a new refracting surface. This means that a regular (spherical) rigid contact lens can provide good level of vision in people who have astigmatism or distorted corneal shapes as with keratoconus.
While rigid lenses have been around for about 120 years, soft lenses are a much more recent development. The principal breakthrough in soft lenses made by Otto Wichterle led to the launch of the first soft (hydrogel) lenses in some countries in the 1960s and the approval of the 'Soflens' material (polymacon) by the United States FDA in 1971. Soft lenses are immediately comfortable, while rigid lenses require a period of adaptation before full comfort is achieved. The polymers from which soft lenses are manufactured improved over the next 25 years, primarily in terms of increasing the oxygen permeability by varying the ingredients making up the polymers.
A small number of hybrid rigid/soft lenses exist. An alternative technique is piggybacking of contact lenses, a smaller, rigid lens being mounted atop a larger, soft lens. This is done for a variety of clinical situations where a single lens will not provide the optical power, fitting characteristics, or comfort required.
In 1999, 'silicone hydrogels' became available. Silicone hydrogels have both the extremely high oxygen permeability of silicone and the comfort and clinical performance of the conventional hydrogels. These lenses were initially advocated primarily for extended (overnight) wear, although more recently daily (no overnight) wear silicone hydrogels have been launched.
While it provides the oxygen permeability, the silicone also makes the lens surface highly hydrophobic and less "wettable." This frequently results in discomfort and dryness during lens wear. In order to compensate for the hydrophobicity, hydrogels are added (hence the name "silicone hydrogels") to make the lenses more hydrophilic. However the lens surface may still remain hydrophobic. Hence some of the lenses undergo surface modification processes which cover the hydrophobic sites of silicone. Some other lens types incorporate internal rewetting agents to make the lens surface hydrophilic.
EYE TRAUMA
Physical or chemical injuries of the eye can be a serious threat to vision if not treated appropriately and in a timely fashion. The most obvious presentation of ocular (eye) injuries is redness and pain of the affected eyes. This is not, however, universally true, as tiny metallic projectiles may cause neither symptom. Tiny metallic projectiles should be suspected when a patient reports metal on metal contact, such as with hammering a metal surface. Intraocular foreign bodies do not cause pain because of the lack of nerve endings in the vitreous humour and retina that can transmit pain sensations. As such, general or emergency room doctors should refer cases involving the posterior segment of the eye or intraocular foreign bodies to an ophthalmologist. Ideally, ointment would not be used when referring to an ophthalmologist, since it diminishes the ability to carry out a thorough eye examination.
Eye injury by impact of small plastic body.
Causes
Eye injury by impact of small plastic body.
Flying pieces of wood, metal, glass, stone and other material are notorious for causing much of the eye trauma. Blunt injury by fist (during a drunken brawl), ball (cricket ball, lawn tennis ball), shuttle cock (from Badminton) and other high speed flying objects can strike the eye. Small children may indulge in bow-and-arrow games and firecrackers (respectively common during Dussehra and Diwali festivals in India) which can lead to eye trauma. Road traffic accidents (RTAs) with head and facial trauma may also have an eye injury - these are usually severe in nature with multiple lacerations, shards of glasses embedded in tissues, orbital fractures, severe hematoma and penetrating open-globe injuries with prolapse of eye contents. Other causes of intraocular trauma may arise from workplace tools or even common household implements. The same study concluded that sports-related injuries due to eyeglasses wear were more common in those under the age of 18 and that fall-related injuries due to eyeglasses wear were more common in those aged 65 or more. Although eyeglasses-related injuries do occur, prescription eyeglasses and non-prescription sunglasses have been found to "offer measurable protection which results in a lower incidence of severe eye injuries to those wearing.
LASIK
LASIK (laser-assisted in situ keratomileusis) is a type of refractive laser eye surgery performed by ophthalmologists for correcting myopia, hyperopia, and astigmatism. The procedure is generally preferred to photorefractive keratectomy, PRK, (also called ASA, Advanced Surface Ablation) because it requires less time for the patient's recovery, and the patient feels less pain, overall; however, there are instances where PRK/ASA is medically indicated as a better alternative to LASIK.
Many patients choose LASIK as an alternative to wearing corrective eyeglasses or contact lenses.
Procedure
There are several necessary preparations in the preoperative period. The operation itself is made by creating a thin flap on the eye, folding it to enable remodeling of the tissue underneath with laser. The flap is repositioned and the eye is left to heal in the postoperative period.
Preoperative
Patients wearing soft contact lenses typically are instructed to stop wearing them approximately 5 to 7 days before surgery. One industry body recommends that patients wearing hard contact lenses should stop wearing them for a minimum of six weeks plus another six weeks for every three years the hard contacts had been worn. Before the surgery, the patient's corneas are examined with a pachymeter to determine their thickness, and with a topographer to measure their surface contour. Using low-power lasers, a topographer creates a topographic map of the cornea. This process also detects astigmatism and other irregularities in the shape of the cornea. Using this information, the surgeon calculates the amount and locations of corneal tissue to be removed during the operation. The patient typically is prescribed an antibiotic to start taking beforehand, to minimize the risk of infection after the procedure.
Operation
The operation is performed with the patient awake and mobile; however, the patient typically is given a mild sedative (such as Valium) and anesthetic eye drops.
LASIK is performed in three steps. The first step is to create a flap of corneal tissue. The second step is remodeling of the cornea underneath the flap with laser. Finally, the flap is repositioned.
Complications
The incidence of refractive surgery patients having unresolved complications six months after surgery has been estimated from 3% to 6%. The risk for a patient of suffering from disturbing visual side effects like halos, double vision (ghosting), loss of contrast sensitivity (foggy vision) and glare after LASIK depends on the degree of ametropia before the laser eye surgery and other risk factors. For this reason, it is important to take into account the individual risk potential of a patient and not just the average probability for all patients.
A subconjunctival hemorrhage is a common and minor post-LASIK complication.
Squint (Strabismus)
What is squint (strabismus)?
Squint is a misalignment of the two eyes so that both the eyes are not looking in the same direction. This misalignment may be constant, being present throughout the day, or it may appear sometimes and the rest of the time the eyes may be straight.
It is a common condition among children. It may also occur in adults.
What causes squint?
The exact cause of squint is not really known. The movement of each eye is controlled by six muscles. Each of these muscle acts along with its counterpart in the other eye to keep both the eyes aligned properly. A loss of coordination between the muscles of the two eyes leads to misalignment. This misalignment may be the same in all directions of gaze, or in some conditions the misalignment may be more in one direction of gaze, e.g., in squint due to nerve palsy.
Sometimes a refractive error hypermetropia (long sight) may lead to inward deviation of the eye. Poor vision in an eye because of some other eye disease like cataract, etc. may also cause the eye to deviate. Therefore it is important in all the cases of squint, especially in children, to have a thorough eye checkup to rule out any other cause of loss of vision.
What is binocular vision?
Under normal circumstances, when both the eyes have good vision and they are aligned properly, they focus on the same object. Each of the eyes sends picture of the same object, viewed from a slightly different angle. These two images reach the brain, where they are fused to form a single three-dimensional picture with depth perception. This is known as binocular single vision.
What are the problems with squint?
When the eyes are not aligned properly, each of the eyes is focusing on a different object and sends signal to the brain. These two different images reaching the brain lead to confusion and may have either of the two effects:
A child would ignore the image coming from the deviated eye, and thus sees only one image. But in the process, he loses the depth perception. This suppression of the image from the deviating eye results in poor development of vision in this eye, which is known as amblyopia.
An adult can not ignore the image from either eye, and therefore has double vision. This can be very annoying and may interfere with work.
What are the symptoms of squint?
In a child, the parents may notice the deviation of eyes. It is important to remember that the eyes of a newborn are rarely aligned at birth. Most establish alignment at 3-4 weeks of age. Therefore squint in any child who is more than one month old must be taken seriously and should be evaluated by an ophthalmologist.
Adults may notice double vision, or misalignment of the eyes.
How is squint diagnosed?
The squint is diagnosed by the ophthalmologist. He or she would do a few special tests to confirm the squint, to try and find out the cause and to quantify the amount of deviation. In some cases there may be a false appearance of squint due to broad nasal bridge in a child. An ophthalmologist will be able to differentiate between a true squint and false squint.
What is the treatment for squint?
The aims of treatment of squint in order of importance are:
»
Preserve or restore vision
»
Straighten the eyes
»
Restore binocular vision
First of all, the eyes are checked to see if they have any refractive error that may be responsible for squint. If there is any significant refractive error present, it is treated first. In some cases (accommodative squint) a correction of refractive error is all that may be required to treat squint.
Next the eyes are checked for presence of amblyopia. It is important to treat the amblyopia before the surgery for squint. The parents are explained about the importance of this treatment, as their cooperation is very crucial for the success of this treatment.
The squint is treated by surgery of either one or both the eyes. The surgery involves weakening or strengthening of the relevant muscles to restore the balance and to get a good coordination. In some cases with double vision, prisms may be added in the glasses to ease the symptoms.
When should the squint be treated?
In a child, the treatment of squint and any associated amblyopia should be started as soon as possible. Generally speaking, the younger the age at which amblyopia is treated; the better is the chance of recovery of vision. Remember that the child would never grow out of squint. A delay in treatment may decrease the chances of getting a good alignment and the vision.
Are glasses necessary?
Yes. Surgery can not replace the need for glasses. If the child has significant refractive error, glasses are a must. In some cases wearing glasses may correct squint. In other cases, wearing glasses help the eyes to see clearly. This clear vision is very important for the treatment of amblyopia, and also for maintaining the coordination of eyes, once they have been aligned by surgery.
EYE CARE
Vision is a gift to be cherished. Maintaining good vision and taking care of our eyes is a relatively simple task for the vast majority. In this section, we will learn the art of taking care of our eyes and ensuring perfect sight for the greater part of our lives.
The number of people with visual problems is truly staggering. In a developed country like the United States, it is estimated that more than two million people lose partial vision every year and almost a quarter of this number become totally blind. The figures in India are expected to be several times more than two million.
Why are annual eye examinations important?
Annual eye examinations are strongly recommended for everyone. It also serves as a precaution. The benefits of annual eye examination are that it:
»
Detects near and far sightedness at an early stage
»
Detects astigmatism
»
Detects serious diseases like glaucoma
»
Detects cataracts
»
Detects systemic diseases like diabetes and hypertension
Children for whom eye check-ups are crucial
The annual eye examination is more important in the case of children. More than 75% of a child's learning in the growing years is accomplished by vision and even a slight impairment in the child's vision can lead to a significant delay in the child's intellectual development. While all children need regular eye check-ups, there are certain groups of children who are at greater risk. These include:
»
Children born prematurely
»
Children born into a family that has a history of eye problems such as childhood cataracts, mal-aligned eyes , or eye tumours
»
Children who have parents with health problems such as diabetes
»
Children who have had eye injuries even if the injuries have occurred years ago.
Tips for preserving good sight
Besides an annual eye examination, some simple steps can be followed that can help preserve good sight. They are:
»
Avoid meddling with the eyes as far as possible such as rubbing the eyes often, or squeezing them. If there is significant irritation in the eyes, consult your eye doctor.
»
Avoid looking directly at the sun, welding electrodes or any other source of very bright, intense light.
»
Try to watch television from a minimum of six screen lengths from the set, which is the recommended distance. Also watching television for very long hours every day has been known to cause eyestrain.
»
If you have any systemic diseases like hypertension or diabetes, see your eye doctor right away. The eyes are very often damaged in these conditions and early detection and treatment is crucial.
»
Do not use excessive eyeliners or other makeup material for the eye. Some of these could irritate and cause problems for the eye.
Common symptoms of eye diseases
Some common symptoms of eye diseases are:
»
Diminishing vision. This may be sudden or gradual, persistent or intermittent.
»
Redness and irritation in the eyes
»
Pain within the eyes or headache
»
Double vision
»
Watering of or discharge from the eyes
»
Flashes of light or sparks in vision
»
Sudden prominence of the eyes
»
Spots in vision
CONTACT LENS CARE
Helps clear vision
In order to ensure optimum eye health and to maintain a "fresh lens" vision, you must follow the care and cleaning regimen recommended by your eye care practitioner.
Lack of care and cleaning or improper cleaning of your contact lens will lead to the build-up of protein deposits, other dirt, debris, germs and micro-organisms on your lenses and apart from eye irritation and infection may cause red eye, discomfort, cloudy vision and in severe cases, impaired vision.
How to insert and remove your pair of contact lens easily?
What may at first seem difficult can become easy with a little practice. The following procedures will help you to insert and remove your pair of contact lens easily.
To put your lens on
»
Rinse your lens in a multi-purpose or saline solution.
»
Keep your head up and look straight ahead.
»
Place the lens on the tip of your index finger. Pull down your lower eyelid with your middle finger.
»
Look up steadily at a point above you.
»
Place the lens on the lower white of your eye.
»
Remove your index finger and release the lower lid.
»
Look down. Close your eyes for a moment, and the lens will centre itself.
To take your lens out
»
Put one or two drops of a lubricating or wetting drop in each eye. This will moisten the lenses and make them easier to remove.
»
Look up and pull down lower eyelid your middle finger.
»
Place your finger on the lower edge of your lens.
»
Slide the lens down to the white of your eye.
»
Squeeze the lens lightly between your index finger and thumb and remove gently.
»
If the edges of your lens stick together, place a few drops of saline or multi-purpose solution on the lens and rub gently until the edges separate.
DRY EYES ( COMPUTER SYNDROME )
Keratoconjunctivitis sicca (KCS), also called keratitis sicca, sicca syndrome, xerophthalmia, dry eye syndrome (DES), or simply dry eyes, is an eye disease caused by decreased tear production or increased tear film evaporation commonly found in humans and some animals. Keratoconjunctivitis sicca is Latin and its literal translation is "dryness of the cornea and conjunctiva". It may be helpful to know that "sicca" is part of the English word "desiccate."
Symptoms
Typical symptoms of keratoconjunctivitis are dryness, burning and a sandy-gritty eye irritation that gets worse as the day goes on. Symptoms may also be described as itchy, scratchy, stingy or tired eyes. Other symptoms are pain, redness, a pulling sensation, and pressure behind the eye. There may be a feeling that something, such as a speck of dirt, is in the eye. The resultant damage to the eye surface increases discomfort and sensitivity to bright light. Both eyes usually are affected.
There may also be a stringy discharge from the eyes. Although it may seem strange, dry eye can cause the eyes to water. This can happen because the eyes are irritated. One may experience excessive tearing in the same way as one would if something got into the eye. These reflex tears will not necessarily make the eyes feel better. This is because they are the watery type that are produced in response to injury, irritation, or emotion. They do not have the lubricating qualities necessary to prevent dry eye.
Because blinking coats the eye with tears, symptoms are worsened by activities in which the rate of blinking is reduced due to prolonged use of the eyes. These activities include prolonged reading, computer usage, driving, or watching television. Symptoms increase in windy, dusty or smoky (including cigarette smoke) areas, in dry environments, high altitudes including airplanes, on days with low humidity, and in areas where an air conditioner (especially in a car), fan, heater, or even a hair dryer is being used. Symptoms reduce during cool, rainy, or foggy weather and in humid places, such as in the shower.
Most people who have dry eyes experience mild irritation with no long-term effects. However, if the condition is left untreated or becomes severe, it can produce complications that can cause eye damage, resulting in impaired vision or (rarely) in the loss of vision
Symptom assessment is a key component of dry eye diagnosis - to the extent that many believe dry eye syndrome to be a symptom-based disease. Several questionnaires have been developed to determine a score that would allow for dry eye diagnosis. McMonnies & Ho dry eye questionnaire is the one that is often used in clinical studies of dry eyes. There are 14 questions that can give a score from 0 to 45. Scores above 14.5 are consistent with dry eye diagnosis.
Causes
Any abnormality of any one of the three layers of tears produces an unstable tear film, resulting in symptoms of keratitis sicca.
Diagnosis
Dry eyes can usually be diagnosed by the symptoms alone. Tests can determine both the quantity and the quality of the tears. A slit lamp examination can be performed to diagnose dry eyes and to document any damage to the eye.
A Schirmer's test can measure the amount of moisture bathing the eye. This test is useful for determining the severity of the condition. A five-minute Schirmer's test with and without anesthesia using a Whatman #41 filter paper 5 mm wide by 35 mm long is performed. For this test, wetting under 5 mm with or without anesthesia is considered diagnostic for dry eyes.
If the results for the Schirmer's test are abnormal, a Schirmer II test can be performed to measure reflex secretion. In this test, the nasal mucosa is irritated with a cotton-tipped applicator, after which tear production is measured with a Whatman #41 filter paper. For this test, wetting under 15 mm after five minutes is considered abnormal.
A tear breakup time (TBUT) test measures the time it takes for tears to break up in the eye. The tear breakup time can be determined after placing a drop of fluorescein in the cul-de-sac.
A tear protein analysis test measures the lysozyme contained within tears. In tears, lysozyme accounts for approximately 20 to 40 percent of total protein content.
A lactoferrin analysis test provides good correlation with other tests.
Recently it was described a molecule - Ap4A- which is intrinsic component of the tears. The presence of this molecule is abnormally high in different states of the ocular dryness. This molecule could quantifyied biochemically simply taking one tear sample with a plain Schirmer test. Utilizing this technique is possible to determine the concentrations of Ap4A in the tear of the patients and such way to diagnose in an objective way if the samples are corresponding to dry eye
OCCULOPLASTY
Occuloplastic surgery is a subspecialty of ophthalmology that focuses on problems surrounding the eyeball (the lids, the orbit and the lacrimal system) as well as artificial eyes. The Service also includes a cosmetic surgery unit.
The eyelids and structures around the eye are critical for vision. Injuries, congenital defects, aging changes and tumors affecting the eyelids as well as the tissues and bones surrounding the eyes can cause pain, eye damage, vision loss and disfigurement.
In addition, changes in the eye's appearance can decrease one's ability to interact in social settings and in the workplace. And, the tragic loss of an eye because of injury or disease can decrease one's confidence and impair self-image.
The oculoplastic surgeons at the Eye Institute combine in-depth knowledge of the eye with expertise in reconstructive surgery to treat a broad range of conditions:
At Sankara we perform:
»
Lacrimal Surgery – to deal with lacrimal gland disorders and blocked nasolacrimal duct (watering).
»
Eyelid Surgery - to correct lid disorders such as eyelid malpositions (eg entropion), drooping eyelids (ptosis), eyelid tumours and reconstruction.
»
Orbital Surgery – to manage orbital tumours as well as inflammatory and vascular disorders.
»
Aesthetic Surgery – including blepharoplasty, face lift and the use of botulinum.
Our aim is to provide the highest standard of care for all patients with these disorders.
The cosmetic form of botulinum toxin, often referred to by its product name Botox®, is a popular non-surgical injection that temporarily reduces or eliminates frown lines, forehead creases, crows feet near the eyes and thick bands in the neck.
Studies have also suggested that Botox is effective in relieving migraine headaches, excessive sweating and muscle spasms in the neck and eyes.
Our doctors specially trained in Botox would administer the injections and the actual treatment takes only a few minutes and the Botox takes effect in three to ten days. Our state-of-the-art facility is oriented toward providing patient-friendly care.